When your waters break early, this is called preterm pre-labour rupture of membranes (PPROM).
What is preterm pre-labour rupture of membranes (PPROM)?
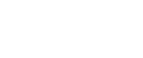
Your baby develops inside a bag of fluid called the amniotic sac. When your baby is ready to be born, the membrane of the amniotic sac breaks. Fluid then comes out through your vagina. This is your waters breaking. It is also known as rupture of the membranes.
Normally your waters break shortly before or during labour. If your waters break before labour at less than 37 weeks of pregnancy, this is called preterm pre-labour rupture of membranes or PPROM.
If this happens, it can (but does not always) trigger early labour. If your waters break early, the risks and your treatment will depend on what stage of your pregnancy you are at.
Is PPROM common in pregnancy?
- PPROM happens in about 3 in every 100 pregnancies.
- PPROM is linked with 3 to 4 out of every 10 premature births.
- About half of pregnant people with PPROM will go into labour within one week of their waters breaking. The further along you are in your pregnancy, the more likely this is to happen.
What causes PPROM?
We do not always know why PPROM happens. It may be caused by one of the following:
- Infection.
- Problems with your placenta. For example where the placenta does not develop properly or is damaged.
- A blood clot develops behind the placenta or membranes.
You may have other risk factors if you:
- have had a premature birth or PPROM before.
- have had any vaginal bleeding during your pregnancy.
- have had any direct trauma (injury) to your stomach.
- have had cervical surgery (such as a large loop excision transformation zone (LLETZ) procedure) or you have a short cervix.
- have had placental abruption before (the placenta does not develop properly or is damaged)
- have extra fluid around your baby in the amniotic sac (known as polyhydramnios).
- are pregnant with more than one baby.
It is important to remember that PPROM is not caused by anything you did or did not do in pregnancy.
How will I know if my waters have broken?
Your waters breaking may feel like a mild popping, followed by a trickle or gush of amniotic fluid that you cannot stop, unlike when you pass urine. The amount of amniotic fluid you lose may vary. You may not feel the actual ‘breaking’. You may only notice your water has broken when you feel the trickle of water. It does not hurt when your waters break.
Amniotic fluid is clear. It may be a little pinkish if it contains some blood. You must call the Maternity Assessment Unit if:
- you think your waters have broken; or
- your waters are smelly or coloured a yellow, brown, or bright red; or
- you are losing fresh blood.
This could mean that you and your baby need to be seen right away.
What happens next?
If your waters have broken, you will often be advised to stay in hospital where you and your baby will be closely monitored for signs of infection. This will be for a few days as this is when you are most likely to go into labour.
- Your temperature, blood pressure, breathing rate and pulse regularly will be checked regularly. You will also have blood tests to check for infection. You will be offered vaginal swabs for vaginal or womb infections. Your team may offer a urine test for a water works infection (urinary tract infection, UTI) and offer antibiotics if needed.
- Your baby’s heart rate will also be monitored regularly.
- You will be offered antibiotics to help reduce the chances of infection.
- If your waters have not broken, you should be able to go home.
What are the risks to PPROM?
Infection
The membranes (amniotic sac) form a protective barrier around your baby. After your membranes break, amniotic fluid can leak out and there is a risk that you may get an infection. This can cause you to go into labour early or cause you or your baby to get sepsis. This is a life-threatening reaction to an infection.
The symptoms of infection are:
- Feeling hot and clammy with shivering.
- An unusual vaginal discharge, with an unpleasant smell.
- A fast heart rate.
- Pain in your lower stomach.
- Feeling generally unwell.
Your baby’s heart rate may also be faster than normal. If there are signs that you have an infection, your baby may need to be born straight away. This is to try to prevent both you and your baby becoming more unwell.

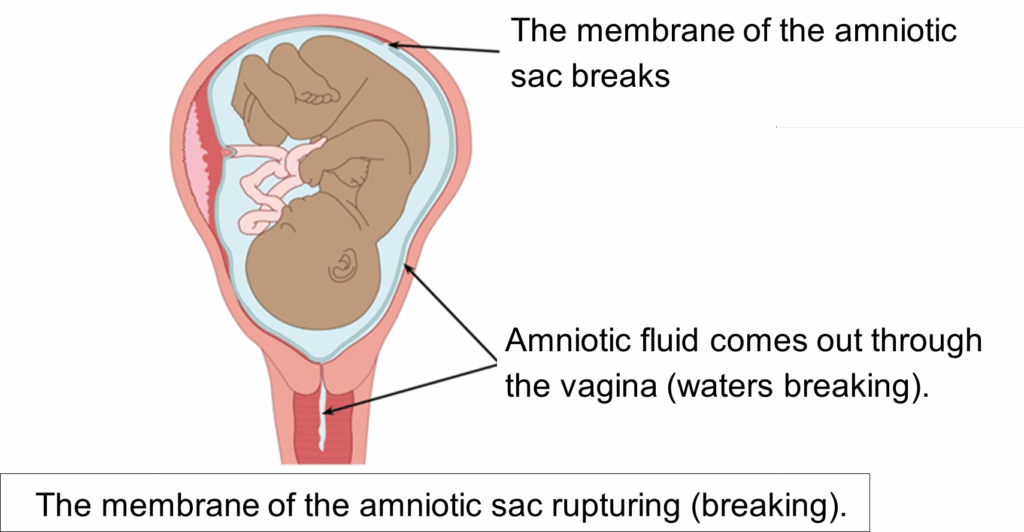
Cord prolapse
This is when the umbilical cord falls through your cervix into your vagina. This is an emergency complication and can be life-threatening for your baby. This risk is uncommon.
Do not try to push the cord back up into the vagina. You should place yourself into a face-down, bottom up in the air, knees to chest position. In the ambulance it is safer for you to lie down on your side.
Follow the position as shown in the image below:

Click here for more information about cord prolapse.
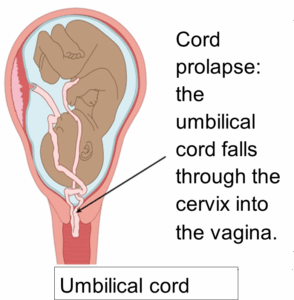
Placental abruption
This is when your placenta separates or starts to separate from your uterus. It can cause pain and heavy bleeding. It can be dangerous for both you and your baby.
This is an emergency and you should get medical attention right away or call 999.
It is important to know that sometimes there can be heavy bleeding with no pain. This happens in 1 in 100 pregnancies. This is more common in pregnancies affected by PPROM.
Pulmonary hypoplasia
This is when your baby’s lungs do not develop normally because they no longer have amniotic fluid around them. This is more common if your waters break very early on in your pregnancy (less than 24 weeks) when your baby’s lungs are still developing.
Are there any treatments for PPROM?
It is not possible to ‘fix’ or heal membranes once they are broken. You may be offered treatment to reduce the risks to your baby. This could include:
- a short course of antibiotics to reduce the risk of an infection.
- a course of steroid injections (corticosteroids) to help with your baby’s lung development. This reduces the chance of problems caused by being born prematurely. Click here for more information about steroids in pregnancy (Easy Read Leaflet)
- magnesium sulphate once you are in labour. This can reduce the risk of your baby developing cerebral palsy if they are born very premature.
- If you do go into premature labour, you will be offered intravenous antibiotics to reduce the risk of early-onset Group B Strep (GBS) infection. The antibiotics are given through a needle straight into a vein. Click here for more information about this.
If you have any questions or concerns about the treatments listed above, please speak to your midwife or doctor.
Do I need to stay in hospital?
It is advised that you to stay in hospital for at least 72 hours (3 days) after your membranes break. This is so the health professionals can monitor you and your baby’s wellbeing. You may be able to go home after that if your doctor thinks that you are not at risk of giving birth early and have no signs of infection.
Before being sent home, you will be given clear advice on how to take your temperature at home.
When should I ask for help if I go home?
Contact the Maternity Assessment Unit and return to the hospital right away if you have any of the following:
- Flu-like symptoms (feeling hot and shivery).
- Bleeding from your vagina.
- The leaking fluid becomes greenish or smelly.
- Contractions or cramping pain.
- Abdominal (stomach) or back pain.
- You are worried that your baby’s movements have slowed down, stopped, or changed.
What follow-up should I have?
After PPROM you should have regular check-ups with a midwife or doctor in a PPROM clinic, often 1 or 2 times a week.
They will monitor your baby’s heart. They will check your temperature, pulse, respiratory rate and blood pressure. You will have blood tests to look for signs of infection. Your team will talk with you about a plan of care for your pregnancy, including regular ultrasound scans to check on your baby’s growth.
When is the right time to give birth?
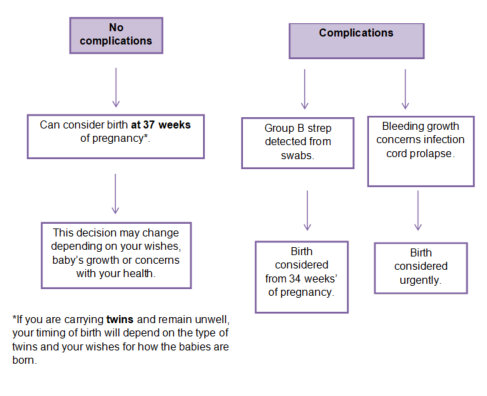
If my baby is going to be born pre-term (born before 37 weeks), how would they be looked after?
There are several treatments that can improve the health of babies born pre-term. The treatments offered depend on how many weeks of pregnancy the baby is at birth.
Click here to view a leaflet that explains these in more detail.
Baby’s health: possible risks and complications
- Pre-term birth: If a baby is born early, there may be short and long term problems with many organs in the body. Some are severe enough to cause death.
- Infection: During labour and after birth, wherever possible doctors will try to treat this with antibiotics. Severe infections can make babies so sick that they can die or have disabilities.
- Breathing problems: Due to the lower amount of water around the baby, the lungs might not develop as well as they should. This can lead to long lasting breathing problems.
- Limb contractures: This is like ‘club foot’ (or hand). Low levels of fluid inside the womb reduce the movement of the baby’s arms and legs and affects their development. Contractures are often treatable with physiotherapy.
For babies born from 27 weeks of pregnancy onwards, the chance of survival is higher. This improves the further along in the pregnancy you are. Your medical team will be able to talk about this with you. Please do still get care if your condition changes even if you are now in more advanced pregnancy. This is because later pregnancies with PPROM can still have complications.
Click here for more about the survival rate of babies born alive between 22 to 26 weeks.
Will I be able to have a vaginal birth after PPROM?
A vaginal birth after PPROM is possible, but it depends on:
- when you go into labour
- the position your baby is in
- your own individual circumstances and choices
Your midwife or doctor will talk about this with you during your care.
Will I have PPROM again with a future pregnancy?
It is likely you will have PPROM or give birth prematurely again. You have an increased risk but it does not mean that you definitely will.
You may be referred to the Premature Prevention Clinic in your next pregnancy.
PPROM under 24 weeks
If your waters break very early (PPROM), sometimes the baby may not survive. This risk is higher if it happens very early in pregnancy if:
- the baby is born before 24 weeks
- there is an infection
- the cord comes out first
If your waters break very early, doctors may talk to you about ending the pregnancy for medical reasons (called termination for medical reasons (TFMR). You would be looked after by specialist teams in maternity and will be offered bereavement and psychological support.
If you feel well and show no signs of infection or labour, you can continue your pregnancy. Due to the risks of complications to both mother and baby, you will also be offered a termination of pregnancy for medical reasons (TFMR).
- Most women opt for medicines to end the pregnancy.
- Some hospitals offer an operation to end the pregnancy. This is less common and may increase risks for your health. It is recommended that you talk with your doctor about this being considered.
Some women with PPROM feel unwell, or their blood tests or heart rate, temperature or blood pressure show an infection is developing. If this happens then you will be offered antibiotics. The option of delivering your baby by the quickest and safest way will be talked about with you, to help you get better.
What if I have any concerns or questions when I return home?
If you have non urgent questions, you will be given the contact details of the PPROM team. If you have any medical concerns, you must contact the Maternity Assessment Unit on 0116 258 6111 for help and advice. They are available 24 hours a day 7 days a week.
More resources
Little Heartbeats is a group that helps women and families going through PPROM. They have 24/7 help available and have a global reach helping women all over the world who experience PPROM. They have a closed Facebook group and website with real life stories. They also provide care packs to help you through PPROM, no matter what choices you make or what happens.
Click here to visit the Little Heartbeats website.

Leicestershire Partnership NHS Trust is responsible for the writing, publishing and updating of the content on this page.
")